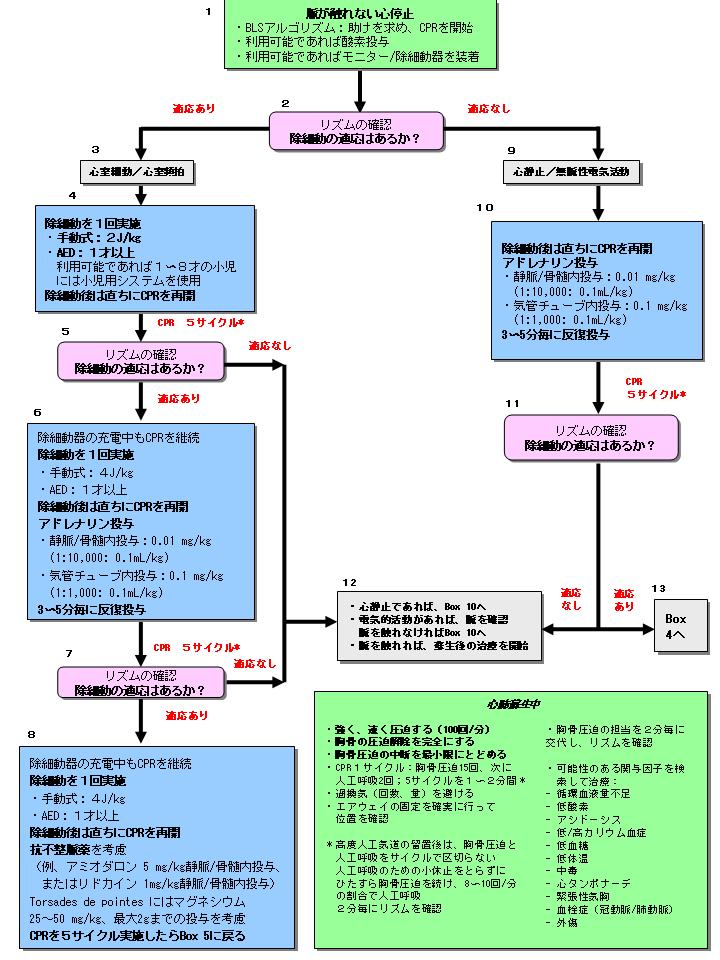
■心停止(Pulseless Arrest)
(PALS Pulseless Arrest Algorithm、原図)
全ての院外心停止小児傷病者のうち、5〜15%に VFが起こる123-125。また小 児院内心停止では蘇生中のいずれかの時点で最大20%に VFが起こると報告さ れている。VFの発生率は年齢と共に上昇する123,125。 除細動は VFの根本的治療である(Class I)。 全体としての生存率は 17〜20%である125-127が、成人で は CPRと除細動をしなければ、生存の可能性は心停止後毎分 7〜 10%低下する128。早期に CPRを実施することで生存率の低下はより緩やかになる。
除細動器
除細動器は手動式または自動式 (AED)であり、単相性または二相性波形のいずれかが用いられている さらなる情報については第5部:「電気的治療: 自動体外式除細動器、除細動、 カルディオバージョン、ペーシング」を参照。
不整脈と心停止の危険性がある小児を治療する医療施設 (例えば、病院、救 急部) は理想的には小児に適するエネルギー量に調節できる除細動器を装備 すべきである。 AEDのパラメータの多くは 自動的に設定されている。 手動式除細動器を用いる時はいくつかの要素を考慮すべきであり、それらは 以下に強調されている(highlighted below)。
-
パドルサイズ
最も大きいサイズのパドルまたは粘着性電極129-131を使用し、胸壁上によく密着させ、パドル同 士が接触しないようにする(パドルの間は約 3cm離す。最良のパドルサイズは
- >10 kg(おおよそ 1歳を超える年齢)の小児には成人用パドル (8〜10 cm)を
- 体重が 10 kg未満の乳児には乳児用パドルを
インターフェース
電極―胸壁間の接着方式(the electrode-chest wall interface)として、ゲルパッド、電極クリーム、ペースト、もしく は粘着式モニター・除細動用パッドを使用することが できる。 生理食塩水に浸したパッド、超音波検査用ゲル、裸のパドルもしくはアル コールパッドは使用しない。
パドル位置
手動式の場合、上胸部右側と心尖部(乳頭の左側で左下部肋骨面)に置いたパドルをしっかり 圧着する(apply firm pressure)。代替の部位としては一方の電極(訳者註:パドル) を胸骨の左隣の前胸壁に、他方を肩甲骨の下の上背部に置132。
投与エネルギー
乳児や小児に対する除細動のエネルギ−量に関して、有効な最 小レベルと安全な最大レベルについてはわかっていない。 4J/kgを超える(9J/kgまで)のエネルギー量で、小児133-135 と幼弱動物モデル136に対してほとんど副作用なく有効に、除細動でき ることが報告されている。 成人での研究37,138や幼弱動物モデルのデータによると、二相性ショックは 単相性ショックと比較して少なくとも同程度に有効であり、有害作用は より少ない。 手動式除細動器(単相性または二相性)では、初回の試みは 2 J/kgのエネルギー量で行い (Class IIa; LOE 5142; 6136)、引き続き試 みる場合は 4 J/kgとする(Class Indeterminate)。
AED
多くの AEDはあらゆる年齢の小児143-145の VFを正確に検出し、高い感度と 特異度でショックの適応と非適応を判別可能である143,144。 ECCガイドライン 2000の出版以来、AEDは 1〜8歳の小児に対して、安全 かつ有効に使用できるというデータが示されてきた143-146。 乳児(1歳未満)への AED使用を推奨する、また はこれに反対するための十分なデータはない(Class Indeterminate)146。 約 1〜8歳の小児に AEDを使用する場合は、エネルギー量を小児に適した 量に低減する、小児用低減装置を使う (Class IIb; LOE 5136; 6139,141)。 小児用低減装置付きの AEDがない場合は標準 AEDを使用するが、小児のショ ック適応波形に対して感度、特異度とも良好なものが好ましい。 小児のケアを行い AEDプログラムがある医療機関には、小児のショック適応リ ズムに対して高い特異度を有し、かつ小児用 低減装置を備えている AEDを使用することが奨められる。
除細動の手順 (Boxes 4, 5, 6, 7, 8)
以下のように考えることが重要である。
- 直ちに除細動を試みる。 除細動を早く試みるほど成功しやすい。
- 除細動器を用いたショックの準備が整うまで CPRを 行い、ショック実施後は直ちに胸骨圧迫から CPRを再開する。 胸骨圧迫の中断は最小限にする。 遷延した成人の心停止147,148と動物モデル134,149では、 その前の胸骨圧迫が有効であるほど除細動に成功する 可能性が高い。 胸骨圧迫の中断は理想的には、換 気(高度気道確保がされるまで)、波形確認そしてショック実施時だけに とどめる。 救助者は波形確認後、除細動器充電中にも(可能ならば)胸骨圧迫を 行う。
- できるだけ速く、ショック(2J/kg)を 1回行い、直ちに胸骨圧迫から CPRを再開 する (Box 4)。 二相性除細動器の初回ショック成功率は 90%を超える150。 初回ショックで VFを除細動できなければ、さらに続けてショックを行うこと の利点は小さく、CPRを再開することにより大きな価値があるだろう。 CPRによっていくらかの酸素と基質を含んだ冠灌流が発生し、引き続き行われるショック で除細動される可能性が高くなる。 胸骨圧迫の中断からショックの実施までの間隔とショックの実施から胸骨圧 迫再開までの間隔を最小限にすることが重要である。 波形を確認する(Box 5)。CPRを 5サイクル続ける(約 2分)。 院内で持続的モニタリング(例えば心電図や血行動態モニター)がされている場合、 上記の手順は医師の裁量によって変更してもよい(第7部(2):「心停 止の管理」を参照)。
-
波形を確認する(Box 5)。
ショック適応の波形が続いている場合は、ショック(4 J/kg)を 1度行い、
直ちに胸骨圧迫を再開する。
アドレナリン(エピネフリン)を 1回投与する。これは波形確認後、
できるだけ早く投与する。
3人目の救助者がいる場合、波形確認の前から、確認後できるだけ早く投与できるよう
に、アドレナリンの準備をするとよい。
CPR中の薬物投与は、除細動器の充電中または通電直後に行う。
しかし、薬物投与のタイミングよりも胸骨圧迫の中断を最小限にすることの方が
より重要である。
アドレナリンの初回および追加投与量としては、 標準的な量を用いる(Class IIa; LOE 4)151。 高用量のアドレナリンをルーチンに使用しても生存に有用 ではなく、特に窒息(訳者註:窒息性心停止)に対しては有害と なる可能性がある(Class III; LOE 2, 4)151。 β-ブロッカー過量投与のような例外的な状況では高用量アドレナリンを考慮してもよい(Class IIb)。 心停止中は標準投与量のアドレナリンを約 3〜5分毎に投与する。
- 5サイクル (約 2分) のCPR後、波形を確認する(Box 7)。 波形が依然として「ショックの適応」であれば、ショック(4 J/kg)を行い、 直ちに CPR(胸骨圧迫からの)を再開し、そしてアミオダロン(Class IIb; LOE 3, 7)103,152-154を投与するか、アミオダロンがなければ CPRを行い ながらリドカインを投与する(Box 8)。 5サイクル(約 2分間)の CPRを続けた後に再び波形を確認し、 必要ならば 4 J/kgで除細動を試みる(Box 6に戻る)。
- 高度気道確保がされれば、2名の救助者は CPRのサイクル(つまり、換気の ために胸骨圧迫を中断すること)をしない。 その代わり、胸骨圧迫担当者は換気のために中断することなく、毎分 100 回の速さで胸骨圧迫を続ける。 換気担当者は毎分 8〜10回の人工呼吸を行う。 2名以上の救助者がいれば、胸骨圧迫担当者の疲労と胸骨圧迫の質や速度が 低下することを避けるため、約 2分毎に胸骨圧迫の担当を交代する。
- 心電計(monitor)や波形 表示できる AEDを使用でき、まとまりのある波形が認めら れた場合は必ず脈の確認を行い、脈の有無に応じて次に進む(Box 12)。
- 除細動成功後に VFが再発した場合は、再 度アミオダロンを投与しながら CPRを続け、前回成功したショックのエネルギ ー量で除細動を試みる(Box 8参照)。
- 治療可能な原因を究明して治療する(緑の「CPR中」boxを参照)。
この多形性 VTは QT間隔が延長している患児に見られ、先天性の可能性 があり、またはIA型抗不整脈薬(例えば、プロカインアミド、キニジ ン、とジソピラミド)やIII型抗不整脈薬(例えば、ソタロールとアミオダロ ン)、三環系抗うつ薬(下記参照)、ジギタリス薬の中毒や薬物相互作用の 結果出現することがある155,156。 アルゴリズム中の緑色のボックスに誘因の例がリストしてある。
治療
原因のいかんに関わらず、硫酸マグネシウムの急速 静注(数分かけて)でトルサードドポアンツを治 療する。
乳児と小児の心停止で最もよく見られる心電図所見は心静止と無脈性電気活 動(PEA)である。PEAは脈を触知しないまとまりのある電気活動(organized electrical activity)(最も一般的には徐脈でQRS幅が広い)であ る。頻度は少ないが、突然の心拍出量の低下 の初期には正常な波形でありながら末梢循環が不良で脈拍を触知できないことがある。 この群(以前は伝導収縮解離(EMD)として知られていた)は治療できる 可能性がより高い。 心静止と PEAへの対応は以下の通りである。
- 胸骨圧迫の中断をできる限り少なくなるように CPRを再開し 継続する(Box 10)。 1人目の救助者が CPRを続けている間に 2人目はアドレナリンを投与する。 心室細動/無脈性 VTと同様、ルーチンに高用量で投与しても生存率の改善はなく むしろ有害である可能性がある。この傾向は特に窒息性(asphyxia)(訳者註:窒息性心停止) の場合により明かである (Class III; LOE 2151; 699,157,158; 7159)。 初回および追加投与には標準的な投与量を用いる(Class IIa; LOE 4)151を用いる。 β遮断薬過量投与のような例外的状 況では高用量アドレナリンを考慮してもよい(Class IIb)。
- 治療可能な原因を究明して治療する(緑色のboxを参照)。
■徐脈(Bradycardia)
(PALS Bradycardia Algorithm、PALS Bradycardia Algorithm原図)
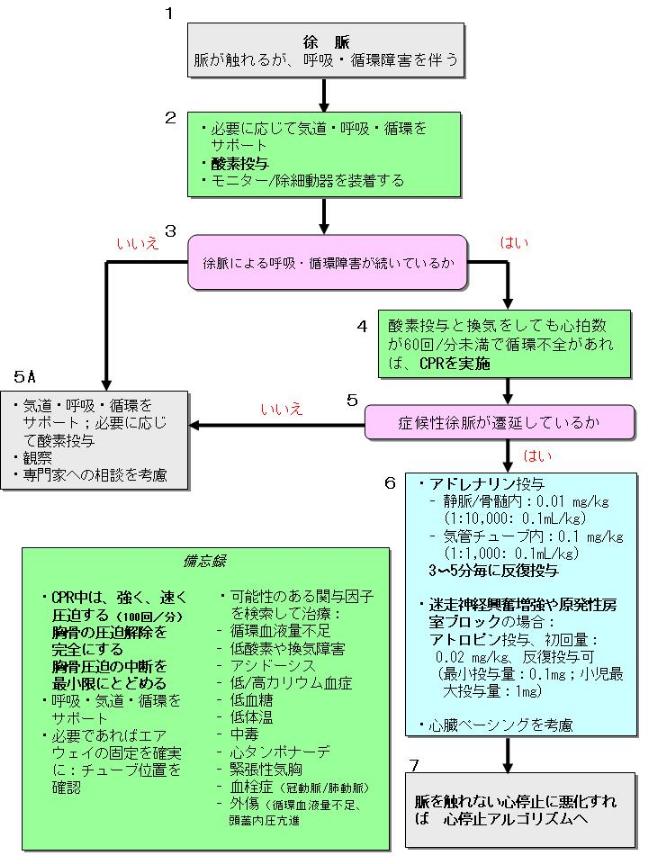
徐脈の緊急治療は徐脈が循環にどの程度の影響を
及ぼしているかによって決まる。
- このアルゴリズムは徐脈によって呼吸・循環不全をきたしている患児のケ アに適用される(Box 1)。 患児が心停止になった場合にはいつでも、小児二次救命処置(PALS)心停 止アルゴリズムを参照する。
- 必要なら気道、呼吸、循環を補助し、酸素を投与し、モニターか除細動器 を装着する(Box 2)。
- 適切な酸素化と呼吸の補助にも関わらず、徐脈がまだ呼吸・循環症状の原因になっているか どうかを判断するために、患児を再評価する(Box 3)。
- 脈、循環、呼吸が正常であれば緊急治療は不要である。 患児をモニタ−し評価を進める(Box 5A)。
- 酸素を用いた効果的な換気にも関わらず、心拍数が 60/min 未満で末梢循環不全があれば、胸骨 圧迫を開始する(Box 6)。
- 適切な酸素化および換気による補助と(適応がある場合)胸骨 圧迫をしていても循環不全の徴候が続いているのかどうかを判断するた めに、患児を再評価する(Box 5)。 補助が適切であることを確認する。例えば、気道および酸素源、そして 換気の効果を確認する。
-
投薬とペーシング(Box 6)
- 気道、換気、酸素化の補助を続け(必要があれば胸骨圧迫も)、 アドレナリンを投与する(Class IIa; LOE 7,8)。 徐脈が続いたり、一時的にしか反応しない場合、 アドレナリンやイソプロテレノールの持続投与を考慮する。
- 徐脈が迷走神経刺激によるものであれば、アトロピンを投与する(Class I) (Box 6)。 徐脈が換気、酸素化、胸骨圧迫および薬剤に反応しない 完全心ブロックや洞房結節機能不全、特に先天性あるいは後 天性の心疾患と関連している場合は、緊急経皮的ペーシングが救命的となる可 能性がある(Class IIb; LOE 5,7160。 ペーシングは心静止160,161、心停止後の低酸素性または 虚血性の心筋障害が原因の徐脈や呼吸不全には有用ではない。
上室性頻拍(SVT)と洞性頻拍を鑑別する上で 12誘導心電
図の評価(Box 3)、患児の臨床所見と病歴(Box 4, 5)が役に立つ。
洞性頻拍であれば、回復可能な原因を探して治療する。
上室性頻拍である可能性が高い頻拍 (Box 5)
治療効果を評価するために心電図をモニターする。
治療法は患児の血行動態がどの程度不安定かによって決まる。
循環不全のある広いQRS幅の頻脈はおそらく心室性由来であるが、変行伝導を
伴った上室性頻拍の可能性もある。
全ての不整脈治療には重篤な副作用の可能性があるため、循環動態的に安定
している小児を治療する前に、小児不整脈の専門家に相談する。
外傷蘇生のいくつかの状況について強調しておく必要がある。
なぜなら不適切に行なわれた蘇生は、防ぎえる小児死亡の主な原因だからで
ある174。
外傷小児の蘇生においてよくある誤りには、気道の開放と
維持ができない場合、蘇生時の輸液管理が不適切である場合、そして
内出血(internal bleeding)の認識と適切な治療ができない場合など
がある。早期から有能な外科医の関与を求め、また多発外傷の患児は可能で
あれば小児の専門家が同乗して、外傷センターへ転送する。
以下は外傷蘇生における特殊な側面である。
下顎挙上法で気道を開通できなければ頭部後屈あご先挙上法で行う。気道は
必ず開通しなければならないからである。
乳児や幼児は頭部が不釣り合いに大きいので、バックボード固定による容認できない頚椎の屈曲を避け
るために、後頭部を埋め込むように固定60したり、体幹を上げたりして、適
切な体位とする必要があるかもしれない59,60。
特別な医療ニーズがある小児182-184は、慢性的な状態(たとえば、気管切開
チューブの閉塞)、補助機器の不具合(たとえば人工呼吸器の不具合)、基
礎疾患の進行、あるいは本来の医療ニーズとは関係のない出来事
185に対して緊急処置が必要になる可能性がある。
CPRに関するさらなる情報については、第11部:「小児の一次救命処置」を参照。
気管切開チューブや気管孔(stoma)を用いた換気
両親、学校看護師(school nurses)、そして在宅介護プロバ
イダー(home healthcare provider)は気道の開通性を評
価し、(訳者註:必要により)これを開通させ、気管切開のある小児の人工気道を用
いて心肺蘇生を行う方法を知っているべきである。
両親と医療従事者(providers)は気管切開チューブから換気をし、胸郭の
拡がりによってその有効性を確認することができなければなら
ない。
チューブを吸引した後も換気できなければチューブを交換する。
もし新品のチューブがなければ、口対気管孔、またはマスク対気管孔換気
を行う。
上気道が開通しているならば、自らまたは他の救助者が気管孔を閉塞することで、
鼻と口から効果的なバッグマスク換気が可能かも知れ
ない。
コカイン、麻薬、三環系抗うつ薬、カルシウム遮断薬、
そしてベータ遮断薬の過量服用は通常の蘇生処置に加えて
他の個別対応を必要とするいくつかの問題をもたらしている(poses
some unique resuscitation problems in addition to the usual
resuscitative measures)。
コカイン
胸痛と不整脈(VF/VTなど)の症状を呈す
る急性冠症候群は成人では最も多い、コカインに関連する入院の理由である186,187。
コカインは活動電位持続時間とQRS幅を延長し、心筋の収縮力を障害する188,189。
治療
三環系抗うつ薬とその他のナトリウムチャンネル遮断薬
中毒量では、心血管系の異常(心室内伝導遅延、心ブロック、徐脈、QT延長、
心室性不整脈(トルサードドポアンツ、VT、VFなど)、低血圧189,197、 痙
攣、そして意識レベルの低下を起こす。
治療
カルシウム遮断薬(Calcium Channel Blockers)
中毒症状として、低血圧、心電図変化(QT間隔の延長、QRS幅の拡大、そし
て右脚ブロック)、不整脈(徐脈、上室性頻拍、心室頻拍、トルサードド
ポアンツ、心室細動)203、意識状態の変化などがある。
治療
ベータ遮断薬(Adrenergic Blockers)
ベータ遮断薬の中毒量では、徐脈、心ブロック、心収縮力の低下が起こる。
QRS幅、QT間隔を延長させる薬剤(プロプラノロール、ソタロール)もある
211-214)。
治療
オピオイド
麻薬は低換気、無呼吸、徐脈、そして低血圧を起こす可能性がある。
治療
適切な血液の酸素化と酸素供給が確認できるまで酸
素投与を続ける。
パルスオキシメータで持続的にモニターする。
重篤な呼吸障害(頻呼吸、不穏や反応の鈍化を伴った呼吸困
難、ガス交換不全、チアノーゼ、低酸素血症)がある場合、気管挿管して
人工呼吸をする。挿管済みの場合はチューブの位置、詰まりがないか(patency)、
きちんと固定されているかを確認する。
院内では、人工呼吸器の最初の設定を行ったり設定を変更した後、
10〜15分後に動脈血ガス分析を行う。
理論的には、血液ガスの値はカプノグラフィーの呼気終末二
酸化炭素濃度と相関しているので、換気の非侵襲的なモニターが可能である。
鎮痛薬(例えばフェンタニルあるいはモルヒネ)や鎮静薬(例えばロラゼパム、
ミダゾラム)で痛みと不快感をコントロールする。
患児が非常に興奮している場合、鎮痛
薬か鎮静薬もしくはこれら両方と神経筋遮断薬(例えばベクロニウムや
パンクロニウム)を併用すると換気が改善し、チューブの位置異常の危険
が減るかもしれない。
しかし、神経筋遮断薬が痙攣をマスクすることがある。
移動や診断手技の間は特に、呼気二酸化炭素をモニターする226。
胃膨満を和らげ予防するために胃管を挿入する。
心拍数、血圧(可能なら直接動脈ラインで)、そして酸素飽和度を持続的にモニターする。
患児が安定するまで、少なくとも 5分ごとに臨床評価を繰り返す。
尿道カテーテルを挿入し、尿量をモニターする。
別に確実な静脈ライン(2ルートを推奨)を確保した後、骨髄ルートを抜去
する。
最低でも、以下の検査を行う。すなわち、
中心静脈血または動脈血のガス分析、電解質、血糖、カルシウム値の
測定である。
胸部レントゲンは気管内チューブの位置、心臓のサイズ、肺の状態の評価に役立つ
だろう。
心拍出量を維持するために用いる薬剤(表2)
低用量(<0.3μg/kg/min)の静注は、一般
的にβアドレナリン作用(強力な変力作用と全身血管抵抗の低下)を、
高用量(>0.3μg/kg/min)ではαアドレナ
リン作用による血管収縮を引き起こす231。
作用には患児によって大きな差があるので、求める効果が
出現するまで投与量を調節する232,233。
アドレナリンは著明な循環の不安定性と非代償性ショックを伴う患児(特
に乳児において)に対して、ドパミンよりも好ましいかもしれない。
ドパミン
輸液に反応せず、全身血管抵抗が低いショックの治療にはドパ
ミンを調節して投与する(Class IIb;LOE 5,6,7)229,234。
典型的には、2〜20μg/kg/minの用量で用いる。
腎血流量を保ち腎機能を改善するために低容量ドパミン投与が
しばしば勧められて来たが、最新の研究ではそのような治療の有効性は示されていない。
ドパミンは高用量(>5μg/kg/min)では心筋のβアドレナ
リン受容体を刺激するが、この効果は乳
児や慢性うっ血性心不全では減弱している可能性がある
231。
20μg/kg/minを超える量の持続投与では、過剰な血管収縮
をきたす可能性がある231。
塩酸ドブタミン
ドブタミンはβ1、β2アドレナリン受容体に選択的に作用し、
心筋収縮力を増し通常末梢血管抵抗を減らす。
特に心筋機能不全236による心拍出量と血圧の低下を改善するた
めに、容量を調節して投与する232,235,236。
ノルアドレナリン(ノルエピネフリン)
ノルアドレナリンは強力な変力作用と末梢血管収縮力のある薬剤である。
輸液に反応しない、全身血管抵抗が低下したショック(敗血症性、
アナフィラキシー性、脊髄性、血管拡張性) の治療のために
容量を調節して投与する。
ニトロプルシドナトリウム
ニトロプルシドナトリウムは血管抵抗(後負荷)を減らすことで心拍出量を
増加させる。
低血圧が心筋機能不全によるものであれば、後負荷を減らすニトロプルシドナトリウム
と心筋収縮力を改善する変力作用薬の併用を考慮する。
強心性血管拡張薬(Inodilators)
強心性血管拡張薬(Inodilators)(イナムリノン、ミルリノン)は心筋の
酸素需要にほとんど影響を与えずに心拍出量を増加させる。
全身または肺血管抵抗の増加した心筋機能不全の治療には、強心性血管拡張薬を
用いる237,239。
血管拡張作用のため輸液が必要となることがある。
強心性血管拡張薬は半減期が長いため、投与速度を変更した後、循環動態に
対する新たな定常状態に達するまでに時間がかかる(イナムリノンは 18時間、
ミルリノンは 4.5時間)。
中毒例では投与を中止しても、有害作用が数時間持続することが
ある。
蘇生の最終目的(goal)の 1つは脳機能を保持する事であ
る。(訳者註:そのために)以下の注意に従い、二次的な神経障害を予防する。
尿量の減少(乳児期(infants)と幼児・学童期(children)では 1 ml/kg/h
未満、 青年期(adolescents)では 30 ml/h未満)は腎前性の原因(例えば脱
水、不十分な全身灌流)、腎臓の虚血による損傷、もしくは複
数の要因が合わさって起こる可能性がある。
腎毒性のある薬剤を避け、腎機能検査が確認できるまでは腎排
泄性の薬剤の用量を調節する。
理想的には、蘇生後のケアは小児集中治療施設の訓練されたチ
ームによって行われるべきである。
蘇生処置が開始されたらできるだけ早く、その様な施設と連絡を取り搬送
について相談する249。
搬送チームのメンバーは重症あるいは外傷患児のケアについて訓練を受け、
十分な経験を持っているべきであり37,250、また小児救急医、小児集中治療
医の指導を受けるべきである。
搬送の方法やチームの構成は個々の患児に必要なケアによっ
て決定する251。
気管挿管された患児の病院間あるいは院内での搬送中には、
呼気二酸化炭素(定性的比色検知器(qualitative
colorimetric detector)またはカプノグラフィー)をモニターする(Class IIa)。
References
1. Young KD, Seidel JS. Pediatric cardiopulmonary resuscitation: a collective
review. Ann Emerg Med. 1999;33:195-205.
2. Gorelick MH, Shaw KN, Murphy KO. Validity and reliability of clinical
signs in the diagnosis of dehydration in children. Pediatrics. 1997;
99:E6.
3. Raju NV, Maisels MJ, Kring E, Schwarz-Warner L. Capillary refill time
in the hands and feet of normal newborn infants. Clin Pediatr. 1999;
38:139 -144.
4. Brown LH, Prasad NH, Whitley TW. Adverse lighting condition effects
on the assessment of capillary refill. Am J Emerg Med. 1994;12:46-47.
5. Park C, Bahk JH, Ahn WS, Do SH, Lee KH. The laryngeal mask airway
in infants and children. Can J Anaesth. 2001;48:413- 417.
6. Bagshaw O. The size 1.5 laryngeal mask airway (LMA) in paediatric
anaesthetic practice. Paediatr Anaesth. 2002;12:420-423.
7. Brown LH, Manring EA, Kornegay HB, Prasad NH. Can prehospital
personnel detect hypoxemia without the aid of pulse oximeters?
Am J Emerg Med. 1996;14:43- 44.
8. Gausche M, Lewis RJ, Stratton SJ, Haynes BE, Gunter CS, Goodrich
SM, Poore PD, McCollough MD, Henderson DP, Pratt FD, Seidel JS.
Effect of out-of-hospital pediatric endotracheal intubation on survival
and neurological outcome: a controlled clinical trial. JAMA. 2000;283:
783-790.
9. Cooper A, DiScala C, Foltin G, Tunik M, Markenson D, Welborn C.
Prehospital endotracheal intubation for severe head injury in children: a
reappraisal. Semin Pediatr Surg. 2001;10:3- 6.
10. Stockinger ZT, McSwain NE Jr. Prehospital endotracheal intubation for
trauma does not improve survival over bag-valve-mask ventilation.
J Trauma. 2004;56:531-536.
11. Pitetti R, Glustein JZ, Bhende MS. Prehospital care and outcome of
pediatric out-of-hospital cardiac arrest. Prehosp Emerg Care. 2002;6:
283-290.
12. Kern KB, Sanders AB, Raife J, Milander MM, Otto CW, Ewy GA. A
study of chest compression rates during cardiopulmonary resuscitation
in humans: the importance of rate-directed chest compressions. Arch
Intern Med. 1992;152:145-149.
13. Aufderheide TP, Sigurdsson G, Pirrallo RG, Yannopoulos D, McKnite
S, von Briesen C, Sparks CW, Conrad CJ, Provo TA, Lurie KG.
Hyperventilation-induced hypotension during cardiopulmonary resuscitation.
Circulation. 2004;109:1960 -1965.
14. Abella BS, Alvarado JP, Myklebust H, Edelson DP, Barry A, O’Hearn
N, Vanden Hoek TL, Becker LB. Quality of cardiopulmonary resuscitation
during in-hospital cardiac arrest. JAMA. 2005;293:305-310.
15. Gausche-Hill M, Lewis RJ, Gunter CS, Henderson DP, Haynes BE,
Stratton SJ. Design and implementation of a controlled trial of pediatric
endotracheal intubation in the out-of-hospital setting. Ann Emerg Med.
2000;36:356 -365.
16. Jesudian MC, Harrison RR, Keenan RL, Maull KI. Bag-valve-mask
ventilation; two rescuers are better than one: preliminary report. Crit
Care Med. 1985;13:122-123.
17. Davidovic L, LaCovey D, Pitetti R. Comparison of 1- vs 2-person
bag-valve-mask techniques for manikin ventilation of infants and
children. Ann Emerg Med. In press.
18. Berg MD, Idris AH, Berg RA. Severe ventilatory compromise due to
gastric distention during pediatric cardiopulmonary resuscitation. Resuscitation.
1998;36:71-73.
19. Moynihan RJ, Brock-Utne JG, Archer JH, Feld LH, Kreitzman TR. The
effect of cricoid pressure on preventing gastric insufflation in infants and
children. Anesthesiology. 1993;78:652- 656.
20. Salem MR, Wong AY, Mani M, Sellick BA. Efficacy of cricoid pressure
in preventing gastric inflation during bag-mask ventilation in pediatric
patients. Anesthesiology. 1974;40:96 -98.
21. Sellick BA. Cricoid pressure to control regurgitation of stomach
contents during induction of anaesthesia. Lancet. 1961;2:404-406.
22. Hartsilver EL, Vanner RG. Airway obstruction with cricoid pressure.
Anaesthesia. 2000;55:208 -211.
23. Sirbaugh PE, Pepe PE, Shook JE, Kimball KT, Goldman MJ, Ward MA,
Mann DM. A prospective, population-based study of the demographics,
epidemiology, management, and outcome of out-of-hospital pediatric
cardiopulmonary arrest [published correction appears in Ann Emerg
Med. 1999;33:358]. Ann Emerg Med. 1999;33:174 -184.
24. Brownstein DR, Quan L, Orr R, Wentz KR, Copass MK. Paramedic
intubation training in a pediatric operating room. Am J Emerg Med.
1992;10:418-420.
25. Vilke GM, Steen PJ, Smith AM, Chan TC. Out-of-hospital pediatric
intubation by paramedics: the San Diego experience. J Emerg Med.
2002;22:71-74.
26. Ma OJ, Atchley RB, Hatley T, Green M, Young J, Brady W. Intubation
success rates improve for an air medical program after implementing the
use of neuromuscular blocking agents. Am J Emerg Med. 1998;16:
125-127.
27. Sing RF, Rotondo MF, Zonies DH, Schwab CW, Kauder DR, Ross SE,
Brathwaite CC. Rapid sequence induction for intubation by an aeromedical
transport team: a critical analysis. Am J Emerg Med. 1998;16:
598-602.
28. Sagarin MJ, Chiang V, Sakles JC, Barton ED, Wolfe RE, Vissers RJ,
Walls RM. Rapid sequence intubation for pediatric emergency airway
management. Pediatr Emerg Care. 2002;18:417- 423.
29. Deakers TW, Reynolds G, Stretton M, Newth CJ. Cuffed endotracheal
tubes in pediatric intensive care. J Pediatr. 1994;125:57- 62.
30. Khine HH, Corddry DH, Kettrick RG, Martin TM, McCloskey JJ, Rose
JB, Theroux MC, Zagnoev M. Comparison of cuffed and uncuffed
endotracheal tubes in young children during general anesthesia. Anesthesiology.
1997;86:627- 631; discussion 27A.
31. Newth CJ, Rachman B, Patel N, Hammer J. The use of cuffed versus
uncuffed endotracheal tubes in pediatric intensive care. J Pediatr. 2004;
144:333-337.
32. Parwani V HI-H, Hsu B, Hoffman RJ. Experienced emergency physicians
cannot safely or accurately inflate endotracheal tube cuffs or
estimate endotracheal tube cuff pressure using standard technique. Acad
Emerg Med. 2004;11:490-491.
33. King BR, Baker MD, Braitman LE, Seidl-Friedman J, Schreiner MS.
Endotracheal tube selection in children: a comparison of four methods.
Ann Emerg Med. 1993;22:530 -534.
34. van den Berg AA, Mphanza T. Choice of tracheal tube size for children:
finger size or age-related formula? Anaesthesia. 1997;52:701-703.
35. Luten RC, Wears RL, Broselow J, Zaritsky A, Barnett TM, Lee T,
Bailey A, Vally R, Brown R, Rosenthal B. Length-based endotracheal
tube and emergency equipment in pediatrics. Ann Emerg Med. 1992;21:
900-904.
36. Katz SH, Falk JL. Misplaced endotracheal tubes by paramedics in an
urban emergency medical services system. Ann Emerg Med. 2001;37:
32-37.
37. Beyer AJ III, Land G, Zaritsky A. Nonphysician transport of intubated
pediatric patients: a system evaluation. Crit Care Med. 1992;20:
961-966.
38. Andersen KH, Schultz-Lebahn T. Oesophageal intubation can be undetected
by auscultation of the chest. Acta Anaesthesiol Scand. 1994;38:
580-582.
39. Kelly JJ, Eynon CA, Kaplan JL, de Garavilla L, Dalsey WC. Use of tube
condensation as an indicator of endotracheal tube placement. Ann Emerg
Med. 1998;31:575-578.
40. Poirier MP, Gonzalez Del-Rey JA, McAneney CM, DiGiulio GA.
Utility of monitoring capnography, pulse oximetry, and vital signs in the
detection of airway mishaps: a hyperoxemic animal model. Am J Emerg
Med. 1998;16:350 -352.
41. Birmingham PK, Cheney FW, Ward RJ. Esophageal intubation: a
review of detection techniques. Anesth Analg. 1986;65:886-891.
42. Donn SM, Kuhns LR. Mechanism of endotracheal tube movement with
change of head position in the neonate. Pediatr Radiol. 1980;9:37- 40.
43. Hartrey R, Kestin IG. Movement of oral and nasal tracheal tubes as a
result of changes in head neck position. Anaesthesia. 1995;50:682- 687.
44. Bhende MS, Thompson AE, Cook DR, Saville AL. Validity of a disposable
end-tidal CO2 detector in verifying endotracheal tube placement
in infants and children. Ann Emerg Med. 1992;21:142-145.
45. Campbell RC, Boyd CR, Shields RO, Odom JW, Corse KM. Evaluation
of an end-tidal carbon dioxide detector in the aeromedical setting. J Air
Med Transp. 1990;9:13-15.
46. Bhende MS, Thompson AE, Orr RA. Utility of an end-tidal carbon
dioxide detector during stabilization and transport of critically ill
children. Pediatrics. 1992;89(pt 1):1042-1044.
47. Bhende MS, Thompson AE. Evaluation of an end-tidal CO2 detector
during pediatric cardiopulmonary resuscitation. Pediatrics. 1995;95:
395-399.
48. Cardoso MM, Banner MJ, Melker RJ, Bjoraker DG. Portable devices
used to detect endotracheal intubation during emergency situations: a
review. Crit Care Med. 1998;26:957-964.
49. Ornato JP, Shipley JB, Racht EM, Slovis CM, Wrenn KD, Pepe PE,
Almeida SL, Ginger VF, Fotre TV. Multicenter study of a portable,
hand-size, colorimetric end-tidal carbon dioxide detection device. Ann
Emerg Med. 1992;21:518 -523.
50. Bhende MS, Karasic DG, Karasic RB. End-tidal carbon dioxide changes
during cardiopulmonary resuscitation after experimental asphyxial
cardiac arrest. Am J Emerg Med. 1996;14:349 -350.
51. Cantineau JP, Merckx P, Lambert Y, Sorkine M, Bertrand C,
Duvaldestin P. Effect of epinephrine on end-tidal carbon dioxide
pressure during prehospital cardiopulmonary resuscitation. Am J Emerg
Med. 1994;12:267-270.
52. Ward KR, Yealy DM. End-tidal carbon dioxide monitoring in
emergency medicine. Part 2: clinical applications. Acad Emerg Med.
1998;5:637- 646.
53. Hand IL, Shepard EK, Krauss AN, Auld PA. Discrepancies between
transcutaneous and end-tidal carbon dioxide monitoring in the critically
ill neonate with respiratory distress syndrome. Crit Care Med. 1989;17:
556-559.
54. Tobias JD, Meyer DJ. Noninvasive monitoring of carbon dioxide during
respiratory failure in toddlers and infants: end-tidal versus transcutaneous
carbon dioxide. Anesth Analg. 1997;85:55-58.
55. Sharieff GQ, Rodarte A, Wilton N, Bleyle D. The self-inflating bulb as
an airway adjunct: is it reliable in children weighing less than 20
kilograms? Acad Emerg Med. 2003;10:303-308.
56. Sharieff GQ, Rodarte A, Wilton N, Silva PD, Bleyle D. The selfinflating
bulb as an esophageal detector device in children weighing
more than twenty kilograms: a comparison of two techniques. Ann
Emerg Med. 2003;41:623- 629.
57. Klain M, Keszler H, Brader E. High frequency jet ventilation in CPR.
Crit Care Med. 1981;9:421- 422.
58. Zander J, Hazinski MF. Pulmonary disorders: airway obstructions. In:
Hazinski MF, ed. Nursing Care of the Critically Ill Child. St. Louis, Mo:
Mosby-Year Book; 1992.
59. Nypaver M, Treloar D. Neutral cervical spine positioning in children.
Ann Emerg Med. 1994;23:208 -211.
60. Herzenberg JE, Hensinger RN, Dedrick DK, Phillips WA. Emergency
transport and positioning of young children who have an injury of the
cervical spine. The standard backboard may be hazardous. J Bone Joint
Surg Am. 1989;71:15-22.
61. Duncan BW, Ibrahim AE, Hraska V, del Nido PJ, Laussen PC, Wessel
DL, Mayer JE Jr, Bower LK, Jonas RA. Use of rapid-deployment
extracorporeal membrane oxygenation for the resuscitation of pediatric
patients with heart disease after cardiac arrest. J Thorac Cardiovasc
Surg. 1998;116:305-311.
62. Morris MC, Wernovsky G, Nadkarni VM. Survival outcomes after
extracorporeal cardiopulmonary resuscitation instituted during active
chest compressions following refractory in-hospital pediatric cardiac
arrest. Pediatr Crit Care Med. 2004;5:440-446.
63. Kanter RK, Zimmerman JJ, Strauss RH, Stoeckel KA. Pediatric
emergency intravenous access. Evaluation of a protocol. Am J Dis Child.
1986;140:132-134.
64. Fiser DH. Intraosseous infusion. N Engl J Med. 1990;322:1579 -1581.
65. Banerjee S, Singhi SC, Singh S, Singh M. The intraosseous route is a
suitable alternative to intravenous route for fluid resuscitation in
severely dehydrated children. Indian Pediatr. 1994;31:1511-1520.
66. Guy J, Haley K, Zuspan SJ. Use of intraosseous infusion in the pediatric
trauma patient. J Pediatr Surg. 1993;28:158 -161.
67. Berg RA. Emergency infusion of catecholamines into bone marrow.
Am J Dis Child. 1984;138:810-811.
68. Andropoulos DB, Soifer SJ, Schreiber MD. Plasma epinephrine concentrations
after intraosseous and central venous injection during cardiopulmonary
resuscitation in the lamb. J Pediatr. 1990;116:312-315.
69. Johnson L, Kissoon N, Fiallos M, Abdelmoneim T, Murphy S. Use of
intraosseous blood to assess blood chemistries and hemoglobin during
cardiopulmonary resuscitation with drug infusions. Crit Care Med.
1999;27:1147-1152.
70. Abdelmoneim T, Kissoon N, Johnson L, Fiallos M, Murphy S.
Acid-base status of blood from intraosseous and mixed venous sites
during prolonged cardiopulmonary resuscitation and drug infusions. Crit
Care Med. 1999;27:1923-1928.
71. Orlowski JP, Porembka DT, Gallagher JM, Lockrem JD, VanLente F.
Comparison study of intraosseous, central intravenous, and peripheral
intravenous infusions of emergency drugs. Am J Dis Child. 1990;144:
112-117.
72. Warren DW, Kissoon N, Sommerauer JF, Rieder MJ. Comparison of
fluid infusion rates among peripheral intravenous and humerus, femur,
malleolus, and tibial intraosseous sites in normovolemic and hypovolemic
piglets. Ann Emerg Med. 1993;22:183-186.
73. Fleisher G, Caputo G, Baskin M. Comparison of external jugular and
peripheral venous administration of sodium bicarbonate in puppies. Crit
Care Med. 1989;17:251-254.
74. Ward JTJ. Endotracheal drug therapy. Am J Emerg Med. 1983;1:71- 82.
75. Johnston C. Endotracheal drug delivery. Pediatr Emerg Care. 1992;8:
94-97.
76. Efrati O, Ben-Abraham R, Barak A, Modan-Moses D, Augarten A,
Manisterski Y, Barzilay Z, Paret G. Endobronchial adrenaline: should it
be reconsidered? Dose response and haemodynamic effect in dogs.
Resuscitation. 2003;59:117-122.
77. Jasani MS, Nadkarni VM, Finkelstein MS, Mandell GA, Salzman SK,
Norman ME. Effects of different techniques of endotracheal epinephrine
administration in pediatric porcine hypoxic-hypercarbic cardiopulmonary
arrest. Crit Care Med. 1994;22:1174 -1180.
78. Lubitz DS, Seidel JS, Chameides L, Luten RC, Zaritsky AL, Campbell
FW. A rapid method for estimating weight and resuscitation drug
dosages from length in the pediatric age group. Ann Emerg Med. 1988;
17:576 -581.
79. Hofer CK, Ganter M, Tucci M, Klaghofer R, Zollinger A. How reliable
is length-based determination of body weight and tracheal tube size in
the paediatric age group? The Broselow tape reconsidered. Br J Anaesth.
2002;88:283-285.
80. Schierhout G, Roberts I. Fluid resuscitation with colloid or crystalloid
solutions in critically ill patients: a systematic review of randomised
trials. BMJ. 1998;316:961-964.
81. Human albumin administration in critically ill patients: systematic
review of randomised controlled trials. Cochrane Injuries Group Albumin
Reviewers. BMJ. 1998;317:235-240.
82. Alderson P, Schierhout G, Roberts I, Bunn F. Colloids versus crystalloids
for fluid resuscitation in critically ill patients. In: The Cochrane
Library. Oxford: England: Update Software. 2003.
83. Longstreth WT Jr, Copass MK, Dennis LK, Rauch-Matthews ME, Stark
MS, Cobb LA. Intravenous glucose after out-of-hospital cardiopulmonary
arrest: a community-based randomized trial. Neurology. 1993;43:
2534-2541.
84. Cherian L, Goodman JC, Robertson CS. Hyperglycemia increases brain
injury caused by secondary ischemia after cortical impact injury in rats.
Crit Care Med. 1997;25:1378 -1383.
85. Simma B, Burger R, Falk M, Sacher P, Fanconi S. A prospective,
randomized, and controlled study of fluid management in children with
severe head injury: lactated Ringer’s solution versus hypertonic saline.
Crit Care Med. 1998;26:1265-1270.
86. Bunn F, Roberts I, Tasker R, Akpa E. Hypertonic versus isotonic
crystalloid for fluid resuscitation in critically ill patients. In: The
Cochrane Library. Oxford, England: Update Software. 2003.
87. Losek JD, Endom E, Dietrich A, Stewart G, Zempsky W, Smith K.
Adenosine and pediatric supraventricular tachycardia in the emergency
department: multicenter study and review. Ann Emerg Med. 1999;33:
185-191.
88. Overholt ED, Rheuban KS, Gutgesell HP, Lerman BB, DiMarco JP.
Usefulness of adenosine for arrhythmias in infants and children.
Am J Cardiol. 1988;61:336 -340.
89. Getschman SJ, Dietrich AM, Franklin WH, Allen HD. Intraosseous
adenosine: as effective as peripheral or central venous administration?
Arch Pediatr Adolesc Med. 1994;148:616-619.
90. Friedman FD. Intraosseous adenosine for the termination of supraventricular
tachycardia in an infant. Ann Emerg Med. 1996;28:356 -358.
91. Somberg JC, Bailin SJ, Haffajee CI, Paladino WP, Kerin NZ, Bridges D,
Timar S, Molnar J. Intravenous lidocaine versus intravenous amiodarone
(in a new aqueous formulation) for incessant ventricular tachycardia.
Am J Cardiol. 2002;90:853- 859.
92. Holt DW, Tucker GT, Jackson PR, Storey GC. Amiodarone pharmacokinetics.
Am Heart J. 1983;106:840-847.
93. Dauchot P, Gravenstein JS. Effects of atropine on the electrocardiogram
in different age groups. Clin Pharmacol Ther. 1971;12:274 -280.
94. Zwiener RJ, Ginsburg CM. Organophosphate and carbamate poisoning
in infants and children [published correction appears in Pediatrics.
1988;81:683]. Pediatrics. 1988;81:121-126.
95. Stueven HA, Thompson B, Aprahamian C, Tonsfeldt DJ, Kastenson EH.
Lack of effectiveness of calcium chloride in refractory asystole. Ann
Emerg Med. 1985;14:630-632.
96. Broner CW, Stidham GL, Westenkirchner DF, Watson DC. A prospective,
randomized, double-blind comparison of calcium chloride and
calcium gluconate therapies for hypocalcemia in critically ill children.
J Pediatr. 1990;117:986 -989.
97. Niemann JT, Criley JM, Rosborough JP, Niskanen RA, Alferness C.
Predictive indices of successful cardiac resuscitation after prolonged
arrest and experimental cardiopulmonary resuscitation. Ann Emerg Med.
1985;14:521-528.
98. Sanders A, Ewy G, Taft T. Prognostic and therapeutic importance of the
aortic diastolic pressure in resuscitation from cardiac arrest. Crit Care
Med. 1984;12:871- 873.
99. Berg RA, Otto CW, Kern KB, Sanders AB, Hilwig RW, Hansen KK,
Ewy GA. High-dose epinephrine results in greater early mortality after
resuscitation from prolonged cardiac arrest in pigs: a prospective, randomized
study. Crit Care Med. 1994;22:282-290.
100. Losek JD. Hypoglycemia and the ABC’S (sugar) of pediatric resuscitation.
Ann Emerg Med. 2000;35:43- 46.
101. Agus MSD, Jaksic T. Nutritional support of the critically ill child
(review). Curr Opin Pediat. 2002;14:470-481.
102. Bigger JT Jr, Mandel WJ. Effect of lidocaine on the electrophysiological
properties of ventricular muscle and purkinje fibers. J Clin Invest.
1970;49:63-77.
103. Dorian P, Cass D, Schwartz B, Cooper R, Gelaznikas R, Barr A.
Amiodarone as compared with lidocaine for shock-resistant ventricular
fibrillation. N Engl J Med. 2002;346:884-890.
104. Wilson FC, Harpur J, Watson T, Morrow JI. Adult survivors of severe
cerebral hypoxia- case series survey and comparative analysis. Neuro
Rehabilitation. 2003;18:291-298.
105. Thomson PD, Melmon KL, Richardson JA, Cohn K, Steinbrunn W,
Cudihee R, Rowland M. Lidocaine pharmacokinetics in advanced heart
failure, liver disease, and renal failure in humans. Ann Intern Med.
1973;78:499 -508.
106. Allegra J, Lavery R, Cody R, Birnbaum G, Brennan J, Hartman A,
Horowitz M, Nashed A, Yablonski M. Magnesium sulfate in the
treatment of refractory ventricular fibrillation in the prehospital setting.
Resuscitation. 2001;49:245-249.
107. Hassan TB, Jagger C, Barnett DB. A randomised trial to investigate the
efficacy of magnesium sulphate for refractory ventricular fibrillation.
Emerg Med J. 2002;19:57- 62.
108. Thel MC, Armstrong AL, McNulty SE, Califf RM, O’Connor CM.
Randomised trial of magnesium in in-hospital cardiac arrest. Duke
Internal Medicine Housestaff. Lancet. 1997;350:1272-1276.
109. Luedtke SA, Kuhn RJ, McCaffrey FM. Pharmacologic management of
supraventricular tachycardias in children. Part 1: Wolff-
Parkinson-White and atrioventricular nodal reentry. Ann Pharmacother.
1997;31:1227-1243.
110. Luedtke SA, Kuhn RJ, McCaffrey FM. Pharmacologic management of
supraventricular tachycardias in children, part 2: atrial flutter, atrial
fibrillation, and junctional and atrial ectopic tachycardia. Ann Pharmacother.
1997;31:1347-1359.
111. Weil MH, Rackow EC, Trevino R, Grundler W, Falk JL, Griffel MI.
Difference in acid-base state between venous and arterial blood during
cardiopulmonary resuscitation. N Engl J Med. 1986;315:153-156.
112. Steedman DJ, Robertson CE. Acid-base changes in arterial and central
venous blood during cardiopulmonary resuscitation. Arch Emerg Med.
1992;9:169 -176.
113. Wayne MA, Delbridge TR, Ornato JP, Swor RA, Blackwell T. Concepts
and application of prehospital ventilation. Prehosp Emerg Care. 2001;
5:73-78.
114. Mattar JA, Weil MH, Shubin H, Stein L. Cardiac arrest in the critically
ill. II. Hyperosmolal states following cardiac arrest. Am J Med. 1974;
56:162-168.
115. Aufderheide TP, Martin DR, Olson DW, Aprahamian C, Woo JW,
Hendley GE, Hargarten KM, Thompson B. Prehospital bicarbonate use
in cardiac arrest: a 3-year experience. Am J Emerg Med. 1992;10:4 -7.
116. Bishop RL, Weisfeldt ML. Sodium bicarbonate administration during
cardiac arrest. Effect on arterial pH PCO2, and osmolality. JAMA.
1976;235:506 -509.
117. Mann K, Berg RA, Nadkarni V. Beneficial effects of vasopressin in
prolonged pediatric cardiac arrest: a case series. Resuscitation. 2002;52:
149-156.
118. Wenzel V, Krismer AC, Arntz HR, Sitter H, Stadlbauer KH, Lindner
KH. A comparison of vasopressin and epinephrine for out-of-hospital
cardiopulmonary resuscitation. N Engl J Med. 2004;350:105-113.
119. Stiell IG, Hebert PC, Wells GA, Vandemheen KL, Tang AS, Higginson
LA, Dreyer JF, Clement C, Battram E, Watpool I, Mason S, Klassen T,
Weitzman BN. Vasopressin versus epinephrine for inhospital cardiac
arrest: a randomised controlled trial. Lancet. 2001;358:105-109.
120. Lindner KH, Dirks B, Strohmenger HU, Prengel AW, Lindner IM, Lurie
KG. Randomised comparison of epinephrine and vasopressin in patients
with out-of-hospital ventricular fibrillation. Lancet. 1997;349:535-537.
121. Guyette FX, Guimond GE, Hostler D, Callaway CW. Vasopressin
administered with epinephrine is associated with a return of a pulse in
out-of-hospital cardiac arrest. Resuscitation. 2004;63:277-282.
122. Reis AG, Nadkarni V, Perondi MB, Grisi S, Berg RA. A prospective
investigation into the epidemiology of in-hospital pediatric cardiopulmonary
resuscitation using the international Utstein reporting style.
Pediatrics. 2002;109:200 -209.
123. Appleton GO, Cummins RO, Larson MP, Graves JR. CPR and the single
rescuer: at what age should you “call first” rather than “call fast”? Ann
Emerg Med. 1995;25:492- 494.
124. Hickey RW, Cohen DM, Strausbaugh S, Dietrich AM. Pediatric patients
requiring CPR in the prehospital setting. Ann Emerg Med. 1995;25:
495-501.
125. Mogayzel C, Quan L, Graves JR, Tiedeman D, Fahrenbruch C, Herndon
P. Out-of-hospital ventricular fibrillation in children and adolescents:
causes and outcomes. Ann Emerg Med. 1995;25:484-491.
126. Herlitz J, Engdahl J, Svensson L, Young M, Angquist KA, Holmberg S.
Characteristics and outcome among children suffering from out of
hospital cardiac arrest in Sweden. Resuscitation. 2005;64:37- 40.
127. Safranek DJ, Eisenberg MS, Larsen MP. The epidemiology of cardiac
arrest in young adults. Ann Emerg Med. 1992;21:1102-1106.
128. Larsen MP, Eisenberg MS, Cummins RO, Hallstrom AP. Predicting
survival from out-of-hospital cardiac arrest: a graphic model. Ann Emerg
Med. 1993;22:1652-1658.
129. Atkins DL, Sirna S, Kieso R, Charbonnier F, Kerber RE. Pediatric
defibrillation: importance of paddle size in determining transthoracic
impedance. Pediatrics. 1988;82:914 -918.
130. Atkins DL, Kerber RE. Pediatric defibrillation: current flow is improved
by using “adult” electrode paddles. Pediatrics. 1994;94:90 -93.
131. Samson RA, Atkins DL, Kerber RE. Optimal size of self-adhesive
preapplied electrode pads in pediatric defibrillation. Am J Cardiol.
1995;75:544 -545.
132. Garcia LA, Kerber RE. Transthoracic defibrillation: does electrode
adhesive pad position alter transthoracic impedance? Resuscitation.
1998;37:139 -143.
133. Gurnett CA, Atkins DL. Successful use of a biphasic waveform
automated external defibrillator in a high-risk child. Am J Cardiol.
2000;86:1051-1053.
134. Rossano JQ, Schiff L, Kenney MA, Atkins DL. Survival is not correlated
with defibrillation dosing in pediatric out-of-hospital ventricular
fibrillation. Circulation. 2003;108:IV320 -IV321.
135. Atkins D, Jorgenson D. Attenuated pediatric electrode pads for
automated external defibrillator use in children. Resuscitation. 2005;66:
31-37.
136. Berg RA, Chapman FW, Berg MD, Hilwig RW, Banville I, Walker RG,
Nova RC, Sherrill D, Kern KB. Attenuated adult biphasic shocks
compared with weight-based monophasic shocks in a swine model of
prolonged pediatric ventricular fibrillation. Resuscitation. 2004;61:
189-197.
137. Schneider T, Martens PR, Paschen H, Kuisma M, Wolcke B, Gliner BE,
Russell JK, Weaver WD, Bossaert L, Chamberlain D. Multicenter,
randomized, controlled trial of 150-J biphasic shocks compared with
200- to 360-J monophasic shocks in the resuscitation of out-of-hospital
cardiac arrest victims. Circulation. 2000;102:1780 -1787.
138. van Alem AP, Chapman FW, Lank P, Hart AA, Koster RW. A prospective,
randomised and blinded comparison of first shock success of
monophasic and biphasic waveforms in out-of-hospital cardiac arrest.
Resuscitation. 2003;58:17-24.
139. Berg RA, Samson RA, Berg MD, Chapman FW, Hilwig RW, Banville
I, Walker RG, Nova RC, Anavy N, Kern KB. Better outcome after
pediatric defibrillation dosage than adult dosage in a swine model of
pediatric ventricular fibrillation. J Am Coll Cardiol. 2005;45:786 -789.
140. Clark CB, Zhang Y, Davies LR, Karlsson G, Kerber RE. Pediatric
transthoracic defibrillation: biphasic versus monophasic waveforms in
an experimental model. Resuscitation. 2001;51:159 -163.
141. Tang W, Weil MH, Jorgenson D, Klouche K, Morgan C, Yu T, Sun S,
Snyder D. Fixed-energy biphasic waveform defibrillation in a pediatric
model of cardiac arrest and resuscitation. Crit Care Med. 2002;30:
2736-2741.
142. Gutgesell HP, Tacker WA, Geddes LA, Davis S, Lie JT, McNamara
DG. Energy dose for ventricular defibrillation of children. Pediatrics.
1976;58:898 -901.
143. Atkinson E, Mikysa B, Conway JA, Parker M, Christian K, Deshpande
J, Knilans TK, Smith J, Walker C, Stickney RE, Hampton DR, Hazinski
MF. Specificity and sensitivity of automated external defibrillator
rhythm analysis in infants and children. Ann Emerg Med. 2003;42:
185-196.
144. Cecchin F, Jorgenson DB, Berul CI, Perry JC, Zimmerman AA, Duncan
BW, Lupinetti FM, Snyder D, Lyster TD, Rosenthal GL, Cross B,
Atkins DL. Is arrhythmia detection by automatic external defibrillator
accurate for children? Sensitivity and specificity of an automatic
external defibrillator algorithm in 696 pediatric arrhythmias. Circulation.
2001;103:2483-2488.
145. Atkins DL, Hartley LL, York DK. Accurate recognition and effective
treatment of ventricular fibrillation by automated external defibrillators
in adolescents. Pediatrics. 1998;101(pt 1):393-397.
146. Samson RA, Berg RA, Bingham R, Biarent D, Coovadia A, Hazinski
MF, Hickey RW, Nadkarni V, Nichol G, Tibballs J, Reis AG, Tse S,
Zideman D, Potts J, Uzark K, Atkins D. Use of automated external
defibrillators for children: an update: an advisory statement from the
pediatric advanced life support task force, International Liaison Committee
on Resuscitation. Circulation. 2003;107:3250 -3255.
147. Cobb LA, Fahrenbruch CE, Walsh TR, Copass MK, Olsufka M, Breskin
M, Hallstrom AP. Influence of cardiopulmonary resuscitation prior to
defibrillation in patients with out-of-hospital ventricular fibrillation.
JAMA. 1999;281:1182-1188.
148. Wik L, Hansen TB, Fylling F, Steen T, Vaagenes P, Auestad BH, Steen
PA. Delaying defibrillation to give basic cardiopulmonary resuscitation
to patients with out-of-hospital ventricular fibrillation: a randomized
trial. JAMA. 2003;289:1389 -1395.
149. Yakaitis RW, Ewy GA, Otto CW, Taren DL, Moon TE. Influence of
time and therapy on ventricular defibrillation in dogs. Crit Care Med.
1980;8:157-163.
150. Martens PR, Russell JK, Wolcke B, Paschen H, Kuisma M, Gliner BE,
Weaver WD, Bossaert L, Chamberlain D, Schneider T. Optimal
Response to Cardiac Arrest study: defibrillation waveform effects.
Resuscitation. 2001;49:233-243.
151. Perondi M, Reis A, Paiva E, Nadkarni V, Berg RA. A comparison of
high-dose and standard-dose epinephrine in children with cardiac arrest.
N Engl J Med. 2004;350:1722-1730.
152. Kudenchuk PJ, Cobb LA, Copass MK, Cummins RO, Doherty AM,
Fahrenbruch CE, Hallstrom AP, Murray WA, Olsufka M, Walsh T.
Amiodarone for resuscitation after out-of-hospital cardiac arrest due to
ventricular fibrillation. N Engl J Med. 1999;341:871- 878.
153. Perry JC, Fenrich AL, Hulse JE, Triedman JK, Friedman RA, Lamberti
JJ. Pediatric use of intravenous amiodarone: efficacy and safety in
critically ill patients from a multicenter protocol. J Am Coll Cardiol.
1996;27:1246 -1250.
154. Perry JC, Knilans TK, Marlow D, Denfield SW, Fenrich AL, Friedman
RA. Intravenous amiodarone for life-threatening tachyarrhythmias in
children and young adults. J Am Coll Cardiol. 1993;22:95-98.
155. van Haarst AD, van’t Klooster GA, van Gerven JM, Schoemaker RC,
van Oene JC, Burggraaf J, Coene MC, Cohen AF. The influence of
cisapride and clarithromycin on QT intervals in healthy volunteers. Clin
Pharmacol Ther. 1998;64:542-546.
156. Ray WA, Murray KT, Meredith S, Narasimhulu SS, Hall K, Stein CM.
Oral erythromycin and the risk of sudden death from cardiac causes.
N Engl J Med. 2004;351:1089 -1096.
157. Berg RA, Otto CW, Kern KB, Hilwig RW, Sanders AB, Henry CP, Ewy
GA. A randomized, blinded trial of high-dose epinephrine versus
standard-dose epinephrine in a swine model of pediatric asphyxial
cardiac arrest. Crit Care Med. 1996;24:1695-1700.
158. Tang W, Weil MH, Sun S, Noc M, Yang L, Gazmuri RJ. Epinephrine
increases the severity of postresuscitation myocardial dysfunction. Circulation.
1995;92:3089 -3093.
159. Rivers EP, Wortsman J, Rady MY, Blake HC, McGeorge FT, Buderer
NM. The effect of the total cumulative epinephrine dose administered
during human CPR on hemodynamic, oxygen transport, and utilization
variables in the postresuscitation period. Chest. 1994;106:1499 -1507.
160. Beland MJ, Hesslein PS, Finlay CD, Faerron-Angel JE, Williams WG,
Rowe RD. Noninvasive transcutaneous cardiac pacing in children.
Pacing Clin Electrophysiol. 1987;10:1262-1270.
161. Quan L, Graves JR, Kinder DR, Horan S, Cummins RO. Transcutaneous
cardiac pacing in the treatment of out-of-hospital pediatric cardiac
arrests. Ann Emerg Med. 1992;21:905-909.
162. Sreeram N, Wren C. Supraventricular tachycardia in infants: response to
initial treatment. Arch Dis Child. 1990;65:127-129.
163. Aydin M, Baysal K, Kucukoduk S, Cetinkaya F, Yaman S. Application
of ice water to the face in initial treatment of supraventricular
tachycardia. Turk J Pediatr. 1995;37:15-17.
164. Ornato JP, Hallagan LF, Reese WA, Clark RF, Tayal VS, Garnett AR,
Gonzalez ER. Treatment of paroxysmal supraventricular tachycardia in
the emergency department by clinical decision analysis [published correction
appears in Am J Emerg Med. 1990;8:85]. Am J Emerg Med.
1988;6:555-560.
165. Lim SH, Anantharaman V, Teo WS, Goh PP, Tan AT. Comparison of
treatment of supraventricular tachycardia by Valsalva maneuver and
carotid sinus massage. Ann Emerg Med. 1998;31:30 -35.
166. Waxman MB, Wald RW, Sharma AD, Huerta F, Cameron DA. Vagal
techniques for termination of paroxysmal supraventricular tachycardia.
Am J Cardiol. 1980;46:655- 664.
167. Gouin S, Ali S. A patient with chaotic atrial tachycardia. Pediatr Emerg
Care. 2003;19:95-98.
168. Mandapati R, Byrum CJ, Kavey RE, Smith FC, Kveselis DA, Hannan
WP, Brandt B III, Gaum WE. Procainamide for rate control of postsurgical
junctional tachycardia. Pediatr Cardiol. 2000;21:123-128.
169. Wang JN, Wu JM, Tsai YC, Lin CS. Ectopic atrial tachycardia in
children. J Formos Med Assoc. 2000;99:766 -770.
170. Epstein ML, Kiel EA, Victorica BE. Cardiac decompensation following
verapamil therapy in infants with supraventricular tachycardia. Pediatrics.
1985;75:737-740.
171. Kirk CR, Gibbs JL, Thomas R, Radley-Smith R, Qureshi SA. Cardiovascular
collapse after verapamil in supraventricular tachycardia. Arch
Dis Child. 1987;62:1265-1266.
172. Rankin AC, Rae AP, Oldroyd KG, Cobbe SM. Verapamil or adenosine
for the immediate treatment of supraventricular tachycardia. Q J Med.
1990;74:203-208.
173. Benson D Jr, Smith W, Dunnigan A, Sterba R, Gallagher J. Mechanisms
of regular wide QRS tachycardia in infants and children. Am J Cardiol.
1982;49:1778 -1788.
174. Dykes EH, Spence LJ, Young JG, Bohn DJ, Filler RM, Wesson DE.
Preventable pediatric trauma deaths in a metropolitan region. J Pediatr
Surg. 1989;24:107-110.
175. Buunke G, van der Hoeveen JG, Meinders AE. Cerebrovascular reactivity
in comatose patients resuscitated from a cardiac arrest. Stroke.
1997;28:1569 -1573.
176. Muizelaar JP, Marmarou A, Ward JD, Kontos HA, Choi SC, Becker DP,
Gruemer H, Young HF. Adverse effects of prolonged hyperventilation
in patients with severe head injury: a randomized clinical trial. J Neurosurg.
1991;75:731-739.
177. Baskaya MK. Inadvertent intracranial placement of a nasogastric tube in
patients with head injuries. Surg Neurol. 1999;52:426-427.
178. Rutledge R, Sheldon GF, Collins ML. Massive transfusion. Crit Care
Clin. 1986;2:791- 805.
179. Niven MJ, Zohar M, Shimoni Z, Glick J. Symptomatic hypocalcemia
precipitated by small-volume blood transfusion. Ann Emerg Med. 1998;
32:498 -501.
180. Ramenofsky ML, Luterman A, Quindlen E, Riddick L, Curreri PW.
Maximum survival in pediatric trauma: the ideal system. J Trauma.
1984;24:818-823.
181. Luterman A, Ramenofsky M, Berryman C, Talley MA, Curreri PW.
Evaluation of prehospital emergency medical service (EMS): defining
areas for improvement. J Trauma. 1983;23:702-707.
182. McPherson M, Arango P, Fox H, Lauver C, McManus M, Newacheck
PW, Perrin JM, Shonkoff JP, Strickland B. A new definition of children
with special health care needs. Pediatrics. 1998;102:137-140.
183. Newacheck PW, Strickland B, Shonkoff JP, Perrin JM, McPherson M,
McManus M, Lauver C, Fox H, Arango P. An epidemiologic profile of
children with special health care needs. Pediatrics. 1998;102:117-123.
184. Emergency preparedness for children with special health care needs.
Committee on Pediatric Emergency Medicine. American Academy of
Pediatrics. Pediatrics. 1999;104:e53.
185. Spaite DW, Conroy C, Tibbitts M, Karriker KJ, Seng M, Battaglia N,
Criss EA, Valenzuela TD, Meislin HW. Use of emergency medical
services by children with special health care needs. Prehosp Emerg
Care. 2000;4:19 -23.
186. Hollander JE, Hoffman RS, Gennis P, Fairweather P, DiSano MJ,
Schumb DA, Feldman JA, Fish SS, Dyer S, Wax P, et al. Prospective
multicenter evaluation of cocaine-associated chest pain. Cocaine Associated
Chest Pain (COCHPA) Study Group. Acad Emerg Med. 1994;1:
330-339.
187. Brody SL, Slovis CM, Wrenn KD. Cocaine-related medical problems:
consecutive series of 233 patients. Am J Med. 1990;88:325-331.
188. Bauman JL, Grawe JJ, Winecoff AP, Hariman RJ. Cocaine-related
sudden cardiac death: a hypothesis correlating basic science and clinical
observations. J Clin Pharmacol. 1994;34:902-911.
189. Kolecki PF, Curry SC. Poisoning by sodium channel blocking agents.
Crit Care Clin. 1997;13:829-848.
190. Lange RA, Cigarroa RG, Flores ED, McBride W, Kim AS, Wells PJ,
Bedotto JB, Danziger RS, Hillis LD. Potentiation of cocaine-induced
coronary vasoconstriction by beta-adrenergic blockade. Ann Intern Med.
1990;112:897-903.
191. Brogan WCI, Lange RA, Kim AS, Moliterno DJ, Hillis LD. Alleviation
of cocaine-induced coronary vasoconstriction by nitroglycerin. J Am
Coll Cardiol. 1991;18:581-586.
192. Hollander JE, Hoffman RS, Gennis P, Fairweather P, DiSano MJ,
Schumb DA, Feldman JA, Fish SS, Dyer S, Wax P, et al. Nitroglycerin
in the treatment of cocaine associated chest pain- clinical safety and
efficacy. J Toxicol Clin Toxicol. 1994;32:243-256.
193. Hoffman RS, Hollander JE. Evaluation of patients with chest pain after
cocaine use. Crit Care Clin. 1997;13:809-828.
194. Lange RA, Cigarroa RG, Yancy CW Jr, Willard JE, Popma JJ, Sills MN,
McBride W, Kim AS, Hillis LD. Cocaine-induced coronary-artery vasoconstriction.
N Engl J Med. 1989;321:1557-1562.
195. Kerns W II, Garvey L, Owens J. Cocaine-induced wide complex dysrhythmia.
J Emerg Med. 1997;15:321-329.
196. Beckman KJ, Parker RB, Hariman RJ, Gallastegui JL, Javaid JI,
Bauman JL. Hemodynamic and electrophysiological actions of cocaine:
effects of sodium bicarbonate as an antidote in dogs. Circulation. 1991;
83:1799 -1807.
197. Dziukas LJ, Vohra J. Tricyclic antidepressant poisoning. Med J Aust.
1991;154:344 -350.
198. Liebelt EL. Targeted management strategies for cardiovascular toxicity
from tricyclic antidepressant overdose: the pivotal role for alkalinization
and sodium loading. Pediatr Emerg Care. 1998;14:293-298.
199. Teba L, Schiebel F, Dedhia HV, Lazzell VA. Beneficial effect of
norepinephrine in the treatment of circulatory shock caused by tricyclic
antidepressant overdose. Am J Emerg Med. 1988;6:566 -568.
200. Tran TP, Panacek EA, Rhee KJ, Foulke GE. Response to dopamine vs
norepinephrine in tricyclic antidepressant-induced hypotension. Acad
Emerg Med. 1997;4:864-868.
201. Williams JM, Hollingshed MJ, Vasilakis A, Morales M, Prescott JE,
Graeber GM. Extracorporeal circulation in the management of severe
tricyclic antidepressant overdose. Am J Emerg Med. 1994;12:456-458.
202. Larkin GL, Graeber GM, Hollingshed MJ. Experimental amitriptyline
poisoning: treatment of severe cardiovascular toxicity with cardiopulmonary
bypass. Ann Emerg Med. 1994;23:480-486.
203. Ramoska EA, Spiller HA, Winter M, Borys D. A one-year evaluation of
calcium channel blocker overdoses: toxicity and treatment. Ann Emerg
Med. 1993;22:196 -200.
204. Henry M, Kay MM, Viccellio P. Cardiogenic shock associated with
calcium-channel and beta blockers: reversal with intravenous calcium
chloride. Am J Emerg Med. 1985;3:334 -336.
205. Howarth DM, Dawson AH, Smith AJ, Buckley N, Whyte IM. Calcium
channel blocking drug overdose: an Australian series. Hum Exp Toxicol.
1994;13:161-166.
206. Horowitz BZ, Rhee KJ. Massive verapamil ingestion: a report of two
cases and a review of the literature. Am J Emerg Med. 1989;7:624-631.
207. Watling SM, Crain JL, Edwards TD, Stiller RA. Verapamil overdose:
case report and review of the literature. Ann Pharmacother. 1992;26:
1373-1378.
208. Kerns W II, Schroeder D, Williams C, Tomaszewski C, Raymond R.
Insulin improves survival in a canine model of acute beta-blocker
toxicity. Ann Emerg Med. 1997;29:748 -757.
209. Kline JA, Tomaszewski CA, Schroeder JD, Raymond RM. Insulin is a
superior antidote for cardiovascular toxicity induced by verapamil in the
anesthetized canine. J Pharmacol Exp Ther. 1993;267:744 -750.
210. Yuan TH, Kerns WP II, Tomaszewski CA, Ford MD, Kline JA. Insulinglucose
as adjunctive therapy for severe calcium channel antagonist
poisoning. J Toxicol Clin Toxicol. 1999;37:463- 474.
211. Kerns W II, Kline J, Ford MD. Beta-blocker and calcium channel
blocker toxicity. Emerg Med Clin North Am. 1994;12:365-390.
212. Lewis M, Kallenbach J, Germond C, Zaltzman M, Muller F, Steyn J,
Zwi S. Survival following massive overdose of adrenergic blocking
agents (acebutolol and labetalol). Eur Heart J. 1983;4:328 -332.
213. Cruickshank JM, Neil-Dwyer G, Cameron MM, McAinsh J. Beta-adrenoreceptor-
blocking agents and the blood-brain barrier. Clin Sci. 1980;
59(suppl 6):453s- 455s.
214. Weinstein RS. Recognition and management of poisoning with betaadrenergic
blocking agents. Ann Emerg Med. 1984;13:1123-1131.
215. Avery GJD, Spotnitz HM, Rose EA, Malm JR, Hoffman BF. Pharmacologic
antagonism of beta-adrenergic blockade in dogs, I: hemodynamic
effects of isoproterenol, dopamine, and epinephrine in acute propranolol
administration. J Thorac Cardiovasc Surg. 1979;77:267-276.
216. Zaritsky AL, Horowitz M, Chernow B. Glucagon antagonism of calcium
channel blocker-induced myocardial dysfunction. Crit Care Med. 1988;
16:246 -251.
217. Mofenson HC, Caraccio TR, Laudano J. Glucagon for propranolol
overdose. JAMA. 1986;255:2025-2026.
218. Love JN, Hanfling D, Howell JM. Hemodynamic effects of calcium
chloride in a canine model of acute propranolol intoxication. Ann Emerg
Med. 1996;28:1- 6.
219. Haddad LM. Resuscitation after nifedipine overdose exclusively with
intravenous calcium chloride. Am J Emerg Med. 1996;14:602- 603.
220. Mc Guire W, Fowlie PW. Naloxone for narcotic exposed newborn
infants: systematic review. Arch Dis Child Fetal Neonatal Ed. 2003;88:
F308-F311.
221. Chernick V, Manfreda J, DeBooy V, Davi M, Rigalto H, Seshia M.
Clinical trial of naloxone in birth asphyxia. J Pediatr. 1988;113:
519-525.
222. Fischer CG, Cook DR. The respiratory and narcotic antagonistic effects
of naloxone in infants. Anesth Analg. 1974;53:849-852.
223. Kattwinkel J, Niermeyer S, Nadkarni V, Tibballs J, Phillips B, Zideman
D, Van Reempts P, Osmond M. An advisory statement from the
Pediatric Working Group of the International Liaison Committee on
Resuscitation. Middle East J Anesthesiol. 2001;16:315-351.
224. American Academy of Pediatrics Committee on Drugs. Naloxone
dosage and route of administration for infants and children: addendum to
emergency drug doses for infants and children. Pediatrics. 1990;86:
484-485.
225. Mills CA, Flacke JW, Flacke WE, Bloor BC, Liu MD. Narcotic reversal
in hypercapnic dogs: comparison of naloxone and nalbuphine. Can J
Anaesth. 1990;37:238 -244.
226. Tobias JD, Lynch A, Garrett J. Alterations of end-tidal carbon dioxide
during the intrahospital transport of children. Pediatr Emerg Care.
1996;12:249 -251.
227. Kern KB, Hilwig RW, Berg RA, Rhee KH, Sanders AB, Otto CW, Ewy
GA. Postresuscitation left ventricular systolic and diastolic dysfunction:
treatment with dobutamine. Circulation. 1997;95:2610 -2613.
228. Meyer RJ, Kern KB, Berg RA, Hilwig RW, Ewy GA. Post-resuscitation
right ventricular dysfunction: delineation and treatment with dobutamine.
Resuscitation. 2002;55:187-191.
229. Ceneviva G, Paschall JA, Maffei F, Carcillo JA. Hemodynamic support
in fluid-refractory pediatric septic shock. Pediatrics. 1998;102:e19.
230. Levy B, Bollaert PE, Charpentier C, Nace L, Audibert G, Bauer P, Nabet
P, Larcan A. Comparison of norepinephrine and dobutamine to epinephrine
for hemodynamics, lactate metabolism, and gastric tonometric variables
in septic shock: a prospective, randomized study. Intensive Care
Med. 1997;23:282-287.
231. Zaritsky AL. Catecholamines, inotropic medications, and vasopressor
agents. In: Chernow B, ed. The Pharmacologic Approach to the Critically
Ill Patient. 3rd ed. Baltimore, Md: Williams & Wilkins; 1994:
387-404.
232. Berg RA, Padbury JF. Sulfoconjugation and renal excretion contribute
to the interpatient variation of exogenous catecholamine clearance in
critically ill children. Crit Care Med. 1997;25:1247-1251.
233. Fisher DG, Schwartz PH, Davis AL. Pharmacokinetics of exogenous
epinephrine in critically ill children. Crit Care Med. 1993;21:111-117.
234. Ushay HM, Notterman DA. Pharmacology of pediatric resuscitation.
Pediatr Clin North Am. 1997;44:207-233.
235. Habib DM, Padbury JF, Anas NG, Perkin RM, Minegar C. Dobutamine
pharmacokinetics and pharmacodynamics in pediatric intensive care
patients. Crit Care Med. 1992;20:601- 608.
236. Martinez AM, Padbury JF, Thio S. Dobutamine pharmacokinetics and
cardiovascular responses in critically ill neonates. Pediatrics. 1992;89:
47-51.
237. Barton P, Garcia J, Kouatli A, Kitchen L, Zorka A, Lindsay C, Lawless
S, Giroir B. Hemodynamic effects of i.v. milrinone lactate in pediatric
patients with septic shock: a prospective, double-blinded, randomized,
placebo-controlled, interventional study. Chest. 1996;109:1302-1312.
238. Bailey JM, Miller BE, Lu W, Tosone SR, Kanter KR, Tam VK. The
pharmacokinetics of milrinone in pediatric patients after cardiac surgery.
Anesthesiology. 1999;90:1012-1018.
239. Abdallah I, Shawky H. A randomised controlled trial comparing milrinone
and epinephrine as inotropes in paediatric patients undergoing
total correction of tetralogy of Fallot. Egyptian J Anaesthesia. 2003;19:
323-329.
240. Hypothermia After Cardiac Arrest Study Group. Mild therapeutic hypothermia
to improve the neurologic outcome after cardiac arrest. N Engl
J Med. 2002;346:549 -556.
241. Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G,
Smith K. Treatment of comatose survivors of out-of-hospital cardiac
arrest with induced hypothermia. N Engl J Med. 2002;346:557-563.
242. Gluckman PD, Wyatt JS, Azzopardi D, Ballard R, Edwards AD, Ferriero
DM, Polin RA, Robertson CM, Thoresen M, Whitelaw A, Gunn AJ.
Selective head cooling with mild systemic hypothermia after neonatal
encephalopathy: multicentre randomised trial. Lancet. 2005;365:
663-670.
243. Shankaran S, Laptook AR, Ehrenkranz RA, Tyson JE, McDonald SA,
Donovan EF, Fanaroff AA, Poole WK, Wright LL, Higgins RD, Finer
NN, Carlo WA, Duara S, Oh W, Cotten CM, Stevenson DK, Stoll BJ,
Lemons JA, Guillet R, Jobe AH. Whole-body hypothermia for neonates
with hypoxic-ischemic encephalopathy. N Engl J Med. 2005;353:
1574-1584.
244. Zeiner A, Holzer M, Sterz F, Schorkhuber W, Eisenburger P, Havel C,
Kliegel A, Laggner AN. Hyperthermia after cardiac arrest is associated
with an unfavorable neurologic outcome. Arch Intern Med. 2001;161:
2007-2012.
245. Takasu A, Saitoh D, Kaneko N, Sakamoto T, Okada Y. Hyperthermia:
is it an ominous sign after cardiac arrest? Resuscitation. 2001;49:
273-277.
246. Ginsberg MD, Busto R. Combating hyperthermia in acute stroke: a
significant clinical concern. Stroke. 1998;29:529 -534.
247. Hickey RW, Kochanek PM, Ferimer H, Alexander HL, Garman RH,
Graham SH. Induced hyperthermia exacerbates neurologic neuronal
histologic damage after asphyxial cardiac arrest in rats. Crit Care Med.
2003;31:531-535.
248. Shum-Tim D, Nagashima M, Shinoka T, Bucerius J, Nollert G, Lidov
HG, du Plessis A, Laussen PC, Jonas RA. Postischemic hyperthermia
exacerbates neurologic injury after deep hypothermic circulatory arrest.
J Thorac Cardiovasc Surg. 1998;116:780 -792.
249. Henning R. Emergency transport of critically ill children: stabilisation
before departure. Med J Aust. 1992;156:117-124.
250. Edge WE, Kanter RK, Weigle CG, Walsh RF. Reduction of morbidity
in interhospital transport by specialized pediatric staff. Crit Care Med.
1994;22:1186 -1191.
251. Guidelines for the transfer of critically ill patients. Guidelines Committee
of the American College of Critical Care Medicine; Society of
Critical Care Medicine and American Association of Critical-Care
Nurses Transfer Guidelines Task Force. Crit Care Med. 1993;21:
931-937.
252. Barratt F, Wallis DN. Relatives in the resuscitation room: their point of
view. J Accid Emerg Med. 1998;15:109 -111.
253. Boie ET, Moore GP, Brummett C, Nelson DR. Do parents want to be
present during invasive procedures performed on their children in the
emergency department? A survey of 400 parents. Ann Emerg Med.
1999;34:70 -74.
254. Doyle CJ, Post H, Burney RE, Maino J, Keefe M, Rhee KJ. Family participation
during resuscitation: an option. Ann Emerg Med. 1987;16:673-675.
255. Hanson C, Strawser D. Family presence during cardiopulmonary resuscitation:
Foote Hospital emergency department’s nine-year perspective.
J Emerg Nurs. 1992;18:104 -106.
256. Meyers TA, Eichhorn DJ, Guzzetta CE. Do families want to be present
during CPR? A retrospective survey. J Emerg Nurs. 1998;24:400-405.
257. Robinson SM, Mackenzie-Ross S, Campbell Hewson GL, Egleston CV,
Prevost AT. Psychological effect of witnessed resuscitation on bereaved
relatives.[comment]. Lancet. 1998;352:614-617.
258. Boyd R. Witnessed resuscitation by relatives. Resuscitation. 2000;43:171-176.
259. Offord RJ. Should relatives of patients with cardiac arrest be invited to
be present during cardiopulmonary resuscitation? Intensive Crit Care
Nurs. 1998;14:288 -293.
260. Eichhorn DJ, Meyers TA, Mitchell TG, Guzzetta CE. Opening the
doors: family presence during resuscitation. J Cardiovasc Nurs. 1996;
10:59 -70.
261. Zaritsky A, Nadkarni V, Getson P, Kuehl K. CPR in children. Ann
Emerg Med. 1987;16:1107-1111.
262. Lopez-Herce J, Garcia C, Dominguez P, Carrillo A, Rodriguez-Nunez
A, Calvo C, Delgado MA. Characteristics and outcome of cardiorespiratory
arrest in children. Resuscitation. 2004;63:311-320.
263. Lopez-Herce J, Garcia C, Rodriguez-Nunez A, Dominguez P, Carrillo
A, Calvo C, Delgado MA. Long-term outcome of paediatric cardiorespiratory
arrest in Spain. Resuscitation. 2005;64:79-85.
264. del Nido PJ, Dalton HJ, Thompson AE, Siewers RD. Extracorporeal
membrane oxygenator rescue in children during cardiac arrest after
cardiac surgery. Circulation. 1992;86(suppl):II-300 -II-304.
265. Parra DA, Totapally BR, Zahn E, Jacobs J, Aldousany A, Burke RP,
Chang AC. Outcome of cardiopulmonary resuscitation in a pediatric
cardiac intensive care unit. Crit Care Med. 2000;28:3296 -3300.
■頻脈と血行動態の不安定性(Tachycardia and Hemodynamic Instability)
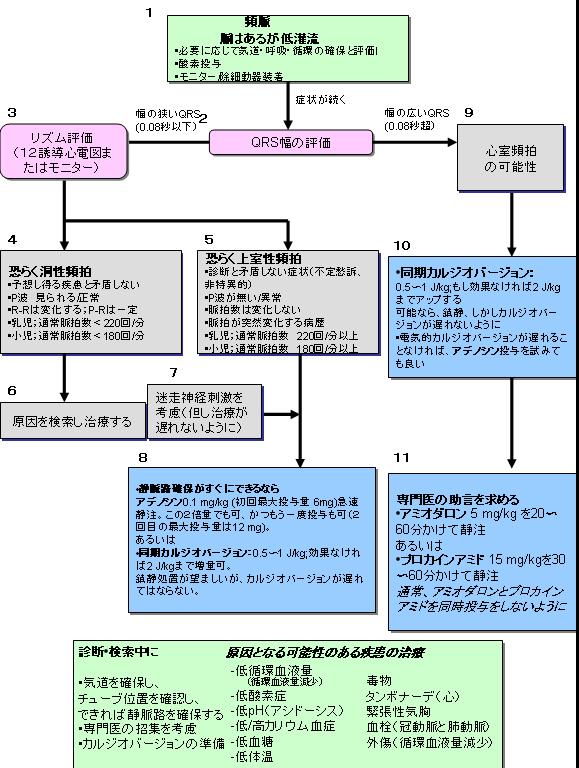
脈が触れなければ、小児二次救命処置(PALS)心停止アルゴリズムに進む。
脈が触れるが循環障害(循環不全、頻呼吸、弱い脈)の徴候があれば、気道
の開通を確認し、必要なら換気を補助し、酸素を投与し、心電図モニターか
除細動器を装着する(Box 1)。
QRS幅を評価(Box 2)する。QRS幅が 0.08秒以下(狭いQRS幅の頻拍)か 0.08秒
より長い(広いQRS幅の頻拍)かを判断する。■特殊な蘇生状況(Special Resuscitation Situations)
■蘇生後の安定化(Postresuscitation Stabilization)
TABLE 2. Medications to Maintain Cardiac Output and for Postresuscitation Stabilization(原表)
薬剤(Medication) 投与量(Dose Range) コメント イナムリノン 0.75〜1 mg/kg IV/IO(5分かけて)。
必要により 2回まで繰り返す。
その後は 2〜20 μg/kg/分で持続静注。 強心血管拡張薬(inodilator) ドブタミン 2〜20 μg/kg/分 IV/IO 強心薬+血管拡張薬 ドパミン 2〜20 μg/kg/分 IV/IO 強心薬+心拍増加薬+腎腸管の血管拡張薬(低用量)/血管収縮薬(高用量) アドレナリン 0.1〜1 μg/kg/分 IV/IO 強心薬+心拍増加薬+血管拡張薬(低用量)/血管収縮薬(高用量) ミルリノン 50〜75 μg/kg IV/IO(10〜60分かけて)、その後は 0.5〜0.75 μg/kg/分で。 強心血管拡張薬(inodilator) ノルアドレナリン 0.1〜2 μg/kg/分 強心薬+血管収縮薬 ニトロプルシドナトリウム 1〜8 μg/kg/分 血管拡張薬、5%糖液(D5W)でのみ希釈可 IV=静注、IO=骨髄内。投与量の他の計算式としては
Infusion rate (mL/h) = [weight (kg) x dose (μg/kg/min) x 60 (min/h)]/concentration μg/mL).
心筋の機能不全は、心停止後によくみられる227,228。
敗血症性ショックの一部の症例を除き、全身および肺血
管抵抗は増加する229。
血管作用薬(vasoactive agents)は血行動態を改善するかもしれないが、臨床的な反応は様々なの
で、それぞれの薬剤と用量を患児に合わせて調節する(Class IIa;LOE 5,6,7)。
血管作用薬は全て確実な静脈ラインから投与する。
カテコラミンの潜在的な副作用には局所の虚血と潰瘍、頻脈、心房性および
心室性頻拍、高血圧、そして代謝の変化(高血糖、乳酸値の上昇230、低カリ
ウム血症)などがある。
■蘇生中の家族の同席
(Family Presence During Resuscitation)■蘇生努力の中止(Termination of Resuscitative Efforts)