
Rescue breating for Infants |
|---|
Mouth to mouth-nose respiration is recommended as cardiopulmonary resuscitation for infants below one year old. However, there had not been enough studies as to whether mouth to mouth-nose artificial respiration is actually possible. Therefore, we have now investigated whether mothers can perform the mouth to mouth-nose artificial respiration on an infant below 1 year old.
[Method]
The following measurements were done for 92 mothers who attended the infant cardiopulmonary resuscitation seminar at the fire department headquarters, and their children were subjects with their mouths closed. In measuring the width of mother's mouth, artificial respiration was actually performed with the lip rouge on and with a gauze on mannequin (resusci-baby); the width of the mouth was measured from the rouge on the gauze. The widths of each mother was also measured with the mouth open.
[Results]
The width of mothers' mouths (A) was 4.5 (0.6) cm, and the directly measured width was 4.3 (0.6) cm. The length B + C + D of infants necessary for the mouth to mouth-nose artificial respiration was 5.6 ( 0.8) cm for those below 6 months old (38 infants), 5.5 (0.4) cm for those below 12 months old (54 infants), and 5.5 (0.4) cm for the mannequins. The length B + C of infants necessary for the mouth to nose artificial respiration was 3.8 (0.6) cm for those below 6 months old, and 3.8 (0.6) cm for those below 12 months old. Also, the number of mothers who could give mouth to mouth-nose artificial respiration to their own child was 7 out of 92 (7.6 %), and those who could give mouth to nose artificial respiration was 74 out of 92 (80.4 %).
Values are shown as mean (standard deviation).
[Conclusion]Mouth to mouth-nose artificial respiration is nearly impossible. Therefore, we need to promote mouth to nose artificial respiration rather than mouth to mouth-nose artificial respiration as the artificial respiration for infants below one year old.
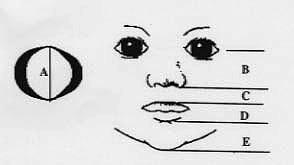
A 4.5 cm (Gauze), 4.3 cm (Direct measurement)
B 2.6 cm (Below 6 months old), 2.7 cm (6-12 months old)
C 1.2 cm (Below 6 months old), 1.2 cm (6-12 months old)
D 1.5 cm (Below 6 months old), 1.8 cm (6-12 months old)
E 1.9 cm (Below 6 months old), 1.8 cm (6-12 months old)
B+C+D 5.4 cm (Below 6 months old), 5.6 cm (6-12 months old)
It is difficult to cover infant's mouth and nose by the mother's
mouth.
B+C 3.8 cm (Below 6 months old), 3.8 cm (6-12 months old)
It is possible to cover infant's nose by the mother's mouth.
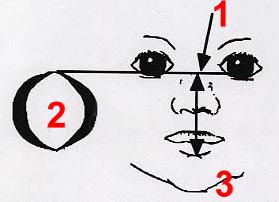
From the above knowledge, it seems better to perform artificial respiration for infants in the following way.
1) One hand performes head tilt while the other hand lifts the infant's jaw
2) Put a corner of the mother's mouth on the upper potion of nose of infant at the height of the intercanthal line.
3) Open the mother's mouth widely and try to cover with her mouth infantŐs nose and mouth.
4) Breathing
Even if the infant's mouth and nose cannot be completely covered, because infant's nose can be covered, rescue breating with mouth to nose technique is possible. Also, the inflow can be adjusted by leaking it from infant's mouth when the inflow is too much.

Remarks: If the corner of the mother's mouth places on the infant's lower lip, and open her mouth widely to cover infant's mouth and nose, mother's mouth will cover down to infant's nose wings. Under this situation infant's nose is obstructed by the mother's mouth and rescure breathing become difficult.